Under the assumption that a majority of the readers of this blog are from the UK, I’m guessing not many have experienced, or even come across Dengue fever, or “breakbone fever” as it is often referred to. Any readers from the USA, central America, Australia, or other parts of the tropics are potentially acutely aware of the disease. The illness is characterised by high fever, malaise and bone/join/muscle pain which can be crippling (hence the colloquial name of breakbone fever). In extreme cases, Dengue can present with hemorrhagic fever (similar to the symptoms of Ebola).
 |
| Aedes mosquito |
Dengue fever is caused by Dengue virus (DENV for ease), which is transmitted by Aedes mosquitoes. As with other mosquito borne diseases, due to global warming, the cases of Dengue fever are increasing because the habitable zone of the mosquitoes is expanding. Currently it is believed that 2.5 billion people are at risk of DENV infection. Currently, there are no approved drugs to directly tackle DENV, nor is there a licensed vaccine, even with intense research in the area. However, recent trials of a potential vaccine, produced by Sanofi-Pasteur have been very promising, and it is this which I will discuss here. I’d first like to tell you a little bit about DENV to explain why producing a vaccine has been so challenging, before looking at the results of the recent clinical trials and the potential for a licensed Dengue vaccine.
 |
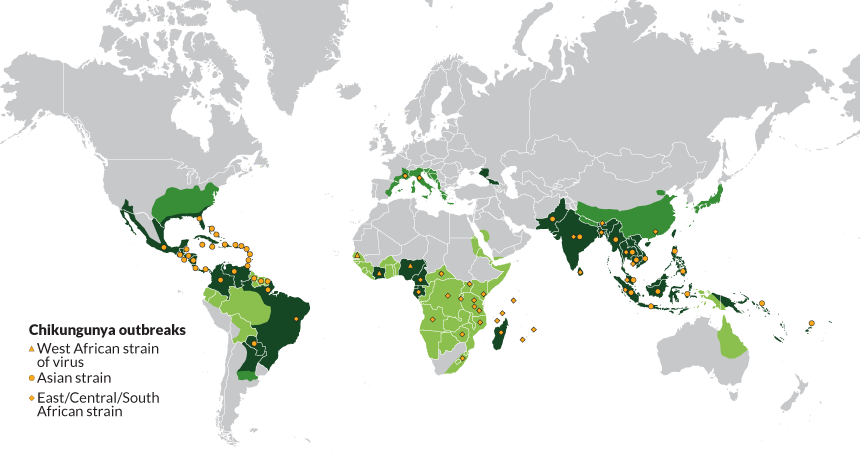
| An image from http://www.healthmap.org/dengue/en/ of the cases of DENV in that last 3 months. Areas closer to red being those with most cases and most confidence. |
DENV is a very interesting virus because of its interplay with the immune system. Let us use the example of measles virus to explain what I mean. When measles virus infects an individual (or they receive the vaccine), the immune response is activated and will produce antibodies specific to that virus. These antibodies bind to the virus and block it from infecting cells and promoting its destruction in immune cells such as macrophage, stopping the infection and protecting you. Those antibodies will do nothing against any other virus, but are very effective against measles.
An antibody response is highly beneficial against certain viruses, such as measles, but the situation is a little more complex for DENV. There are four very distinct types of DENV, which are known as serotypes, DENV-1, -2, -3 and -4. Should an individual become infected by DENV-1, for instance, they will produce protective antibodies against this serotype of the virus. If someone else is infected by DENV-2, they will produce antibodies specific to that virus. Antibodies specific to each serotype are only effective for that particular virus; DENV-2 antibodies will have no protective effect on DENV-1. This production of these specific antibodies is largely what dictates there being four DENV serotypes.
If an individual is infected with DENV-1, they will produce protective antibodies against re-infection by DENV-1. However, if that person should become infected by any of the other DENV serotypes (let’s use DENV-2), this can produce a life threatening situation. The antibodies specific to DENV-1 from the primary infection will bind to DENV-2, but instead of stopping the virus from infecting cells, the antibodies will promote infection of cells that are not normally infected by DENV - a phenomenon known as antibody dependent enhancement (ADE).
 |
| A diagram to depict ADE (from http://www.the-scientist.com/?articles.view/articleNo/34586/title/Antibody-Dependent-Enhanced--ADE--Immunity/). 1) Virus infects cells. 2) The immune response is activated and antibodies produced. 3) These antibodies bind to the virus and can result in uptake to, and 4) destruction in macrophage cells. 5) Upon a secondary infection from a different serotype, 6) antibodies are release from memory B cells. 7) These release antibodies do not bind the new serotype as effectively. 8) The virus can infect more cells, such as macrophages, leading to more extensive infection. |
|
One such example of cells more susceptible to a secondary infection are macrophage cells. Under normal circumstances, a macrophage will detect virus particles bound by antibodies and destroy them. However, in the case of DENV and ADE, the macrophage are unable to destroy the different serotype of the virus, and will instead become infected. Once infected, these cells will eventually be killed, but can also spread the virus to the rest of the body, and even into the brain. This secondary DENV infection can cause much more extensive infection, and as a result, much more severe disease, often characterised by hemorrhagic fever or shock syndrome which can be life threatening.
The case fatality for DENV is only 1-5%, yet with around 50 million infections each year, and 2.5 billion people living in areas at risk from the transmitting mosquitoes, this is still a lot of people. It is speculated that of the fatalities, a large proportion come from a secondary infection.
A vaccine is generally designed to elicit an antibody response. In short, this has been why producing a DENV vaccine has been so difficult. If the vaccine only produces an antibody response against one serotype of the virus (let’s say DENV-1), that patient is then at more risk of having a severe DENV infection than they would be without the vaccine. In order for an effective vaccine against DENV to be produced, an antibody response against all four serotypes of the virus must be produced at once, so as not to leave the individual susceptible to more severe infection. This has proved very difficult.
There have been many failed attempts at producing a DENV vaccine. However, finally it seems like there may be light at the end of the tunnel. As touched on above, the vaccine has been manufactured by Sanofi-Pasteur and it is based on the yellow fever vaccine. The first vaccine ever produced was against smallpox, credited to Edward Jenner. Once the idea of vaccination became established, the next virus on the hit list was yellow fever virus. The vaccine against yellow fever virus is still one of the most effective ever produced. Yellow fever virus and DENV are from the same virus family (the
Flaviviridae), and therefore share many features. The work at Sanofi-Pasteur used the yellow fever vaccine as a backbone for their DENV vaccine (known as CYD-TDV). The yellow fever vaccine was altered to present the immune system with proteins against each of the four DENV serotypes instead of yellow fever virus, then made as a cocktail of all four (a tetravalent vaccine).
The vaccine has so far been trialled on around 31,000 children (who are at most risk of severe DENV) in
South Asia and
Central America and in both regions has been show to be very effective. In the South Asian trial the vaccine had 56.6% efficacy for all DENV infections, and 80.8% efficacy at preventing severe DENV infections, and importantly, showed no substantial safety concerns. While in the Central American trial these equivalent figures stood at 60.8% and 80.3%. While efficacy of around 60% may seem low, this is still a vast improvement from no protection, but most importantly, the vaccine seems to be able to reduce the number of hospitalisations from severe DENV infection by up to 80%.
The vaccine is still yet to be licensed, but with the results from these phase III clinical trials, the prospects look good. Sanofi-Pasteur has already spent
20 years and $1.7 billion in the attempts to bring this drug to market, so not least for them, but also for the 2.5 billion people at risk of DENV infection, the prospects of a DENV vaccine are highly exciting. Hopefully later this year we will see the vaccine on the market.